

Health is Pills
take more and more, get better and better!

If doctors won’t give you pills, it’s a kind of theft: They’re taking health away from you. Fortunately, more injections might help, but what if they give us the injections without also letting us have lots and lots of pills? How are we supposed to be safe and healthy, then?
Matthew Fleischer is a longtime journalist, and the editor of the opinion pages at the San Francisco Chronicle, and a recent victim of a Covid-19 infection. Here’s his recent op-ed piece about it, and do note the subhed:
Doctors made it worse. By not giving him pills.
Now, you probably wouldn’t have imagined that anyone on the planet hasn’t heard about Paxlovid rebound, at this late point, after the President of the United States experienced it, and after Saint Anthony experienced it, but the newspaper editor Matthew Fleischer probably has limited contact with the news, so he must have just missed all of that. And so he knows that Paxlovid would have fixed his Covid, and his doctors made him have to be sick by not doing anything magical to him with the miracle of pills. Fleischer:
I’m hopeful the new omicron booster can break this cycle. But what if it doesn’t?
This begs the question: if an antiviral drug like Paxlovid exists that could potentially ease people’s COVID symptoms by preventing the virus from replicating in our bodies before it spreads, why are we being so precious about who we give it to?
So he contacts a doctor, “UCSF infectious disease specialist Monica Gandhi,” to ask why he wasn’t given Paxlovid. And she tells him — get a load of this anti-science noise! — that Paxlovid is being used to prevent death and hospitalization in the infected, but that “studies of people in my age range have shown no discernible benefits in this regard to taking the drug.” Also, she adds, Fleischer is vaccinated (as if you couldn’t already tell), and “there just have not been any studies on this in vaccinated people.”
She tells him that he’s asking doctors for a pharmaceutical product that hasn’t been tested on people in his condition, and has no proven benefits for people of his age, and his response — as someone who believes in science — is to more or less stomp his feet about it: “Given that the known side effects of Paxlovid are few and mild, some doctors are comfortable bending the rules to prescribe the drug to those who might not technically meet the public health guidance.”
(But daddy, I want it! I want a golden goose!)
He doesn’t want testing, he wants pills. Bend the rules so he can have them, see, even if they don’t technically meet the stupid public health guidance thing and whatever. Try to guess how much the opinion pages of the San Francisco Chronicle have spent the last two and a half years caterwauling for everyone to obey the public health experts. Anyway, did Matthew mention that he WANTS PILLS, because he really really would like you to know about that.
That’s how we got here. That’s how we got a whole bunch of here:

Not mentioned in Fleischer’s piece: Any other intervention that he pursued to bring his infection under control. There are protocols from the doctors at the Frontline Covid-19 Critical Care Alliance, and they suggest a whole bunch of things that might help, starting with Vitamin D and progressing through DON’T EVEN SAY HORSE PASTE YOU NAZI, and even simple aspirin probably helps. My recent Covid-19 infection was a mild cold — I coughed for a whole day. I pulled up the early treatment protocol and did it, with a daily aspirin or two and some Vitamin D and a little of the other thing that you shouldn’t ever take, because it’ll make you listen to Joe Rogan and invade Poland.
For that matter, moderate exercise and fresh air are helpful, so go take a walk.
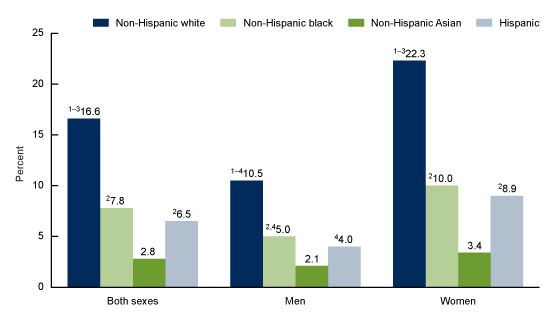
But exercising and taking some Vitamin D isn’t pills, and only pills can make you not be sick. This is especially true if the pills are new, and specially formulated for Current Thing. Bizarrely, there’s a whole bunch of race, class, and gender tangled up in this distinctly consumer-inflected attitude:
We have a frequent and serious discussion about overprescription in America, with doctors and pharmaceutical companies taking most of the well-deserved heat for it. But the consumer demand for MOAR PILLZ is pushy, and here it is in all its glory.
Oh, and one more thing: “I’m hopeful the new omicron booster can break this cycle.” It’s probably the fifth shot that’ll make him safe, but he still wants the pills.
It’s a treadmill. With manacles.
I’m a physician, and every word of what you just wrote resonates with me. I retired about 10 years ago—in my early 40s!—because I just couldn’t take it anymore. Medicine had become something I didn’t recognize (thanks, Obamacare!). Heavy reliance on physician extenders (RNs, NPs, etc.—don’t get me wrong, many are good at what they do, but it’s folly to think their training is equivalent to ours), the push to solve every problem with pharmaceuticals, hospital politics, and the constant wrangling with insurance companies turned a job I enjoyed into a grind that, frankly, wasn’t worth it. So I quit to devote all my time toward something where I could really make a difference: raising my kids. It worked out splendidly—both are happy and thriving, and completely free of psychoactive pharma poison. I’m an empty nester now, but I would never, ever go back into practice. I’m not about to put pronouns on my badge or lecture patients about their privilege.
Decades ago, I was almost tossed out of medical school during my 4th year psychiatry rotation for challenging the narrative around SSRIs. At that time, they were being passed out like candy at Halloween. In clinic, I interviewed patient after patient, none of whom seemed any better over the weeks and months they had spent on the drugs. When I questioned this, ooh boy, did those psychiatrists get mad. I had to defend myself in front of a tribunal at the school for challenging what would now be referred to as “settled science.” So I laughed weeks ago when the news reports of SSRI failure finally came out. The jig is up! But don’t hold your breath—it won’t change anything. SSRIs are here to stay, dug into the fabric of our society like an Alabama tick.
I will say that most docs I know, no matter how reflexively they prescribe pills to others, shun them personally. In my own practice, I tried hard to encourage the simplest, and what I have found for decades myself to be a tried-and-true solution to the blues: go outside. There is something instantly uplifting about being outdoors in nature that makes it harder to stay sad. It might not fix everything, but it’s a helluva better place to start than swallowing a pill.
Forgive me for donning my pedant cap, but Fleischer is a hack. He writes: "This begs the question..." NO. No questions have been begged! Questions have been raised! "Begging the question" is when an argument's premises assume the truth of the conclusion. In other words, a circular argument. People use "beg the question" as a substitute for "raise the question" to, I guess, sound more erudite. NO. Don't do it.